Folic Acid (synthetically produced found in supplements and fortified foods) also called as Folate (naturally found in foods), is a water soluble vitamin, which is also known as Vitamin B9 or Folacin.
Chemistry
The compound consists of three components namely: Pteridine ring, P-amino benzoic acid (PABA) and Glutamic acid. Active form of folic acid is Tetrahydrofolate.
In circulation it is present as N-methyl Tetrahydrofolate.
Properties
Yellowish, slightly water soluble and soluble in alcohol and destroyed by cooking, heat and light & can be precipitated into salts of barium or lead.
Sources of Folic Acid
Rich sources: yeast, meat, liver, fortified foods.
Good: Green leafy vegetables.
Fair: milk and milk products, fruits, bread, banana.
Biochemical Functions of Folic Acid
1.One Carbon metabolism: Tetrahydrofolate is the coenzyme of Folic Acid, and is the integral part of one carbon metabolism. Tetrahydrofolate acts as donor or an acceptor of one carbon units like formyl, methyl, amine etc. in many reactions which involves nucleotide metabolism and amino acid metabolism.
Many important compounds may be synthesized through one carbon metabolism like: Purine and Pyrimidine (nucleotide which are incorporated in DNA), Glycine, serine and choline (different amino acids), N-formylmethonine (initiator of biosynthesis of proteins)
Nucleic acid metabolism: Tetrahydrofolate takes part in metabolism through two different pathways, one by synthesis of the precursors i.e. purine and pyrimidine and the other by synthesis of methionine from homocysteine. Methionine is required for synthesizing S-adenosylmethionine (SAM is a methyl group donor and is mainly used in Methylation reactions specially various sites on DNA and RNA there by controlling gene expression and cell differentiation)
Amino acid metabolism: Folic Acid is involved in synthesis of various amino acids: Methionine, Glycine, Serine and Cysteine.
2.Homocysteine metabolism: It is regulated by three vitamins which are Vitamin B12, Folic Acid and Vitamin B6. Folic acid and Vitamin B 12 acts as a cofactor or a coenzyme for methionine synthesis from homocysteine. Through other pathway vitamin B6 converts homocysteine into other amino acids. Thus these three vitamins together control concentration of homocysteine in blood.

Role of Folic Acid in Disease Prevention
Megaloblastic anemia:

It is a disorder caused by impaired DNA synthesis. In patients with this anemia present with macrocytic red cells bone marrow shows erythroid hyperplasia with abnormal structure.
And immature RBC’s are produce and released into circulation.
This impaired DNA synthesis is due to deficiency of folic acid of Vitamin B12.
Prevents adverse pregnancy outcomes:
During development of the fetus in the womb, there is wide spread cell division for which adequate amount of folic acid is required for formation or synthesis of DNA and RNA. Neural tube defects (NTDs) are life threatening malformations and defects seen in infants (failure of fusion of embryonic neural tubes by 21 to 28 days after fertilization.) e.g. meningomyelocele, encephalocele, anencephaly, spina bifida. It is observed that women who consume Folic Acid during periconceptional period and during pregnancy reduce the chances of NTDs drastically.
Its supplements also reduce the risk of congenital malformations like cleft lip and cleft palate, congenital abnormalities of heart.
Its supplementation during pregnancy is found to increase the birth weight of infants and decrease the risk of low birth weight babies.
Cardiovascular Diseases:
Increase in serum homocysteine levels is associated with atherosclerosis, thrombosis and hypertension. Hyperhomocyteinaemia is due to folate deficiency which may be accompanied with Vitamin B12 & 6 deficiency.
Children having deficiency of one of three enzymes methionine synthase, MTHFR or cystathionine synthase have severe homocystinuria and blood levels of more than 100µmol/L have increased risk of vascular diseases e.g. IHD, cerebrovascular disease or pulmonary embolus either in young adulthood or as teenagers. Trails have sown that when the patients have received Vitamin B12, Folic Acid and Vitamin B6 reduced incidences of vascular diseases and lowering of homocysteine levels.
Cancer:
Folic acid may prevent cancer due to its role in DNA synthesis and gene expression. It is thought to increase thymine pools and thus better quality DNA synthesis as it shunts 1-carbon group towards thymine and Purine synthesis. This explains its association in lowering of risk top colorectal cancer.
Prophylactic folic acid supplements during pregnancy in some and not all, a reduced incidence acute lymphoblastic leukemia (ALL) in childhood.
Folic Acid may feed tumors so it must be avoided in well established tumors.
Alzheimer's disease and cognitive impairment:
Psychiatric disturbances are seen in both folate and cobalamin deficiency. Due to failure of synthesis of SAM, production of neurotransmitters of brain is affected. Link between lower levels of serum folate or cobalamin and higher homocysteine levels and decreased cognitive functions and dementia of Alzheimer's disease is seen.
Deficiency of Folic Acid
Etiology
- Old age, infancy, poverty
- Congenital defects of folate enzymes (e.g. cyclohydrolase or methionine synthase.)
- Dietary intake is inadequate,
- Alcoholism,
- Increased requirement, excess utilization or loss,
- Malabsorption,
- Taking over cooked foods as heat destroys folic acid.
Generally the most known deficiency, usually seen in,
- Pregnant and lactating women due to increased requirements.
- Patients suffering from tropical spur, gluten-induced enteropathy in children and adults malabsorption syndromes such as celiac disease, inflammatory bowel disease (Crohn’s disease), and active liver diseases.
- Certain patients on folic acid antagonists or antifolate drugs like methotrexate (Aminopterin and Amethopterin) and Trimethoprim.
- Increased loss from hemodialysis, peritoneal dialysis.
Clinical Features of Deficiency of Folic Acid
A few patients may be symptomatic or may present with following symptoms
- Patients presents with anemia, glossitis, cheilosis, retarded growth, gastric symptoms like diarrhea, distension and flatulence.
- Severe folate deficiency is also associated with infertility or even sterility in both males and females.
- In early pregnancy may cause abortions or in infants congenital malformations.
Hematological manifestations
- A blood film shows oval Macrocytosis and Hypochromia with elevated MCV (in children it may show Microcytic and Hypochromic anemia) and hypersegmented polymorhonuclear cells.
- The bone marrow is frankly Megaloblastic but in patients with moderate form it may be normoblastic with few megaloblasts.
- Elevated levels of blood Homocysteine levels.
Diagnosis
Diagnosis is based on history and relevant abnormities in peripheral blood film and analysis of serum folic acid levels.
Treatment
- Folic Acid is replaced at doses of 1-5mg/d orally.
- Large doses of Folic Acid are used to treat the Hematological manifestation along with Vitamin B12.
- Folic acid supplements taken during gestation period by pregnant females, helps to prevent neural tube defects and chromosomal abnormalities in the infants.
- Also it should also be given with methotrexate, trimethoprim, pyrimethamine and pentamidine as they are known to impair folate metabolism.
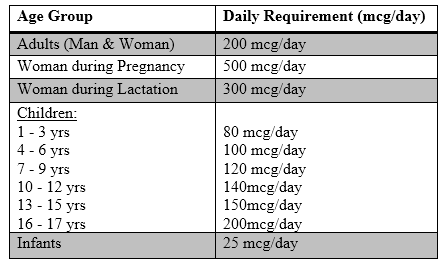
Recommended Dietary Allowances
RDA is 0.5 mg/d.
Requirements of Folic Acid increases during pregnancy, infancy, exfoliative skin diseases (i.e. where cell division is more) and malignancy. Its requirement is greatest when there is rapid cell multiplication.
Toxic effects of over dose of Folic Acid
Usually never seen as it is a water soluble vitamin and is excreted form the when taken in high doses.
References:
- Medical physiology by Guyton and Hall, eleventh edition, chapter 71, page no 877
- Human physiology by Dr. C. C. Chaterjee, eleventh edition, volume one, chapter 11, page no 687
- Harper’s illustrated Biochemistry , 29th edition, section 6 chapter 44, page no 536
- Book on biochemistry by U. Satyanarayana and U. Chakrapani Section 1Chapter 7, page no143
- Parks text book of preventive and social medicine 22nd edition chapter no 11page no 574
- API text book of medicine volume 2 section 15 chapter 4 page no 933
- Davidson text book on medicine 18th edition, Megaloblastic anemia, chapter no. 105, pg no. 864
- https://books.google.co.in/books?hl=en&lr=&id=ja8KAAAAQBAJ&oi=fnd&pg=PP1&dq=folic+acid+its+role+and+functions+in+human+body+from+book+vitamins+their+role+in+human+body&ots=UjAyCfAsEq&sig=gSWJwQlHFHLh77x3mX2Q_8VkYps#v=onepage&q&f=false
- http://www.bourre.fr/pdf/publications_scientifiques/259.pdf
- https://scholar.google.co.in/scholar?q=folic+acid+its+role+and+functions+in+human+body+from+book+vitamins+their+role+in+human+body&btnG=&hl=en&as_sdt=0%2C5
- https://www.google.co.in/search?q=folic+acid&ie=utf-8&oe=utf-8&gws_rd=cr&ei=A3nXVuSfIdDkuQShsqDoBA
- http://lpi.oregonstate.edu/mic/vitamins/folate
- http://www.ncbi.nlm.nih.gov/pubmed/21891867
- http://www.oxfordjournals.org/our_journals/tropej/online/mcnts_ch
- DE GRUCHY & apos; S CLINICAL HAEMATOLOGY IN MEDICAL PRACTICE, 5TH ED - Frank Firkin, Colin Chesterman, Bryan Rush, David Pennigton - Google Books ap9.pdf
- Metzner Theory of Urine Formation - R.A. Kenney - Google Books